Treating Arthritis with Red Light Therapy: A Plain-English Guide Built from Real-World Questions
Living with arthritis can feel like a never-ending loop of flare-ups, morning stiffness, swelling, and the dreaded “bone-on-bone” ache. Sufferers also talk about creaky/“crepitus” knees, hands that won’t grip, weather pain, fatigue/brain fog, and the side-effects of meds (NSAIDs, steroids, DMARDs, biologics).
If you've ever had a flair up that makes you say "I can't get up in the morning", then you are one of over 10 million people in the UK alone in the same boat. Morning stiffness in the first 30- 60 minutes can leave you feeling helpless, and couple that with crunching knees, swollen joints and weakness when trying to grip onto that soaking wet umbrella come September, you are in need of some red light wellness.
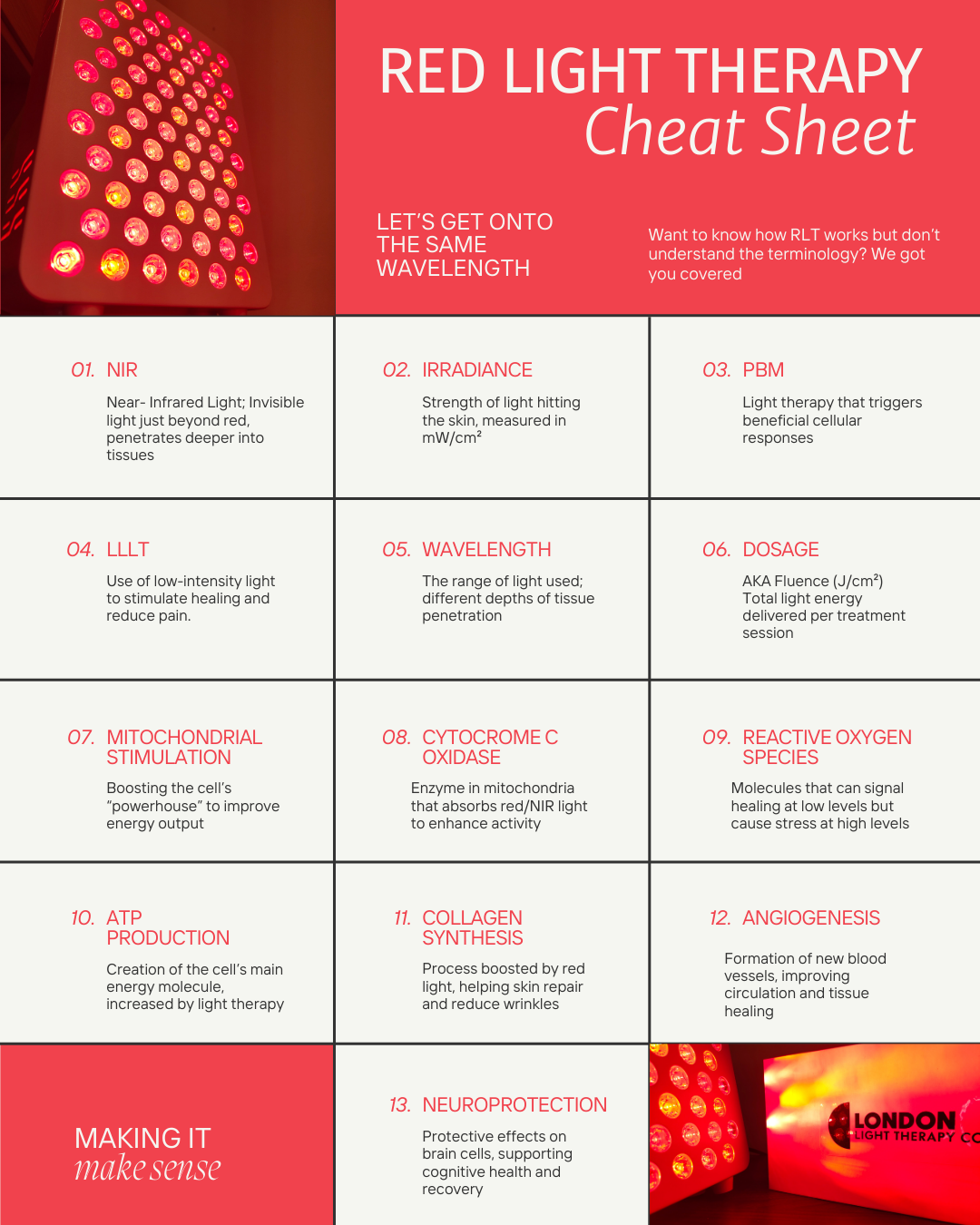
What is red light therapy (photobiomodulation)?
RLT/PBM uses red (~600–700 nm) and near-infrared (NIR, ~800–900 nm) light at low power to nudge cell metabolism (especially mitochondria), reduce inflammatory signalling, and modulate pain. Recent reviews and meta-analyses report meaningful pain and function improvements in knee osteoarthritis in particular, though dosing parameters vary and not every trial is positive.
What the evidence says:
-
Knee OA: Meta-analyses and controlled trials show reduced pain and disability with PBM vs. sham in many studies (not all). Benefits are often larger when PBM is paired with exercise/rehab.
-
Mechanisms: Anti-inflammatory effects and improved microcirculation are repeatedly cited; an umbrella review across PBM indications (2025) rates evidence strength across outcomes and calls for standardised dosing.

How RLT maps to the problems people describe
-
Morning stiffness & “can’t get going”: PBM before activity may help reduce stiffness and ease range-of-motion work (particularly in knees). Pair it with gentle mobility for better effect.
-
Swelling / hot joints in a flare: PBM has anti-inflammatory effects in trials
-
Hand weakness / grip issues: Smaller emitters or wraparound devices can target finger bases and wrists; evidence is strongest in knees, but hands are commonly treated in practice. (Research still catching up.)
- “Bone-on-bone” pain: PBM won’t regrow cartilage, but it may reduce pain, making strengthening and gait retraining more doable.

Will red light therapy let me take less pain medication?
Possibly, for some people—under medical supervision. In RCTs and rehab settings, PBM has reduced pain and improved function, which can lower reliance on analgesics when combined with exercise and good self-management. If you do feel better, talk to your GP/rheumatology team about safely stepping down NSAIDs or other analgesics rather than self-adjusting.
Why be careful? Long-term NSAID or opioid use carries risks, so needing less can be a real health win—but it must be planned to avoid rebound pain or interactions with RA/OA treatment plans. NICE guidance still anchors care on disease-modifying therapy (for RA), exercise/weight management, and judicious analgesia. PBM is an adjunct that may help you hit those goals with fewer pills.
Micro-FAQ (answering common forum questions)
-
“How soon will I feel something?” Some report easier mornings or less “grinding” within 2–3 weeks; others need the full 6-weeks to feel the difference.
-
“Red or near-infrared?” Both appear useful; NIR penetrates a bit deeper (good for knees/hips), while red is common for hands and superficial areas. Mixed devices are best.
- “Can I do this forever?” Most people shift to maintenance (e.g., weekly or during flares) after the initial 3–6 weeks. Since flare- ups can be out of the blue, having a panel at home can really help nip those pains in the bud in record time.
Bottom line
If pain, morning stiffness, swelling, and flare-ups are running your life, red light therapy is a low-risk adjunct with growing evidence—especially for knee osteoarthritis. A 2–3×/week plan over 3–6 weeks is a practical starting point. Combine it with exercise, monitor your response, and work with your doctor if you’re aiming to reduce pain medication for long-term health benefits.
Sources & further reading
-
Meta-analysis & RCT evidence for PBM in knee OA and musculoskeletal rehab. ScienceDirect+3Oxford Academic+3PLOS+3
-
Mechanisms & umbrella review across PBM indications (2025). MDPI+1
-
Emerging clinical practice consensus on PBM use (2025). JAAD
-
Core NHS/NICE guidance for arthritis management (for context alongside any adjunct). NICE+1

{kind=link}
Leave a comment
This site is protected by hCaptcha and the hCaptcha Privacy Policy and Terms of Service apply.